|
Patient 148/1948
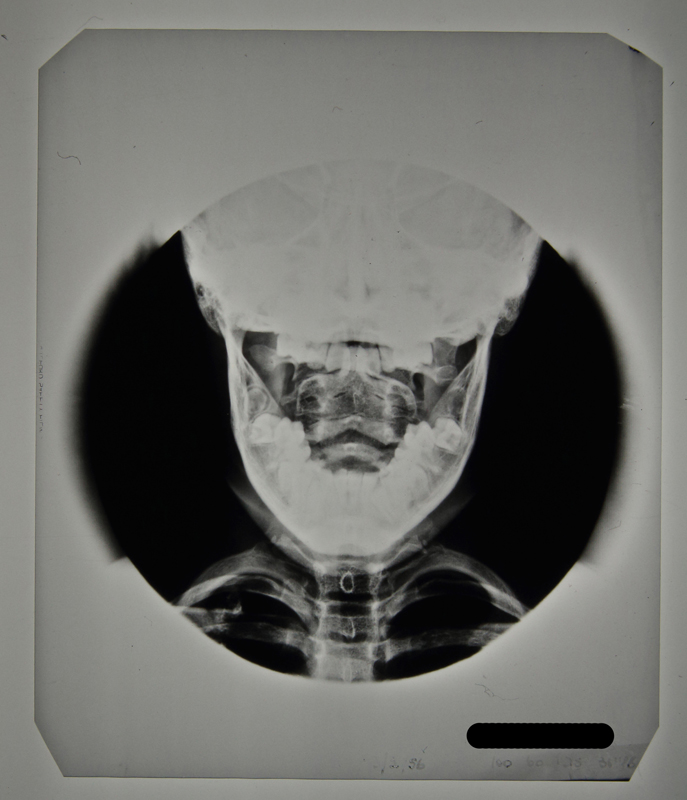
Patient 148/1948 was initially admitted in January 1948 (Patient Number 8/1948) with a Primary Tuberculous Complex of the right mid-zone. However, her initial stay at Stannington was short as she was removed against medical advice by her mother 28 days after admittance, only to be re-admitted seven months later with TB of the cervical spine. Initial observations on re-admission included: "Marked thickening of tissues at back of neck c/o (complaint of) pain in neck but movements fairly good. Limitation of lateral movements more marked to left than right. Marked enlargement of cervical glands."
Following examination with the surgeon, a more comprehensive outline of her condition was given: "The lower surface of the 2nd c.v (cervical vertebrae) is involved; the body of the 3rd c.v is completely destroyed and the upper surface of the 4th is probably eroded. This child should have every bone in her body x-rayed."
It is likely the request for all bones in her body to be x-rayed came from the suspicion that other areas of the skeleton had been affected by the disease. The request was carried out with the x-ray report card indicating that anteroposterior (AP) and lateral radiographs, where possible, were taken of the chest, spine, legs and hips. The patient was immobilised on a Bradford Frame.
Between September and December 1948 the patient is noted to have developed a number of additional symptoms, including vomiting sputum; patchy erythema (a scarlet rash) on her chest; purulent nasopharyngeal discharge (discharging pus from the nose); aural discharge; an inflamed throat and enlarged cervical glands. By July 1949, these symptoms had largely been addressed and the patient was showing improvement. Immobilisation was considered satisfactory as a form of treatment and a moulded plastic splint was to be prepared for the patient, to consist of "a jacket taken from the hips and extending upwards to embrace the head and the occipital region to the chin."
This was later described as being reinforced with steel both vertically and transversely. One year later, further examination by Mr Stanger noted that the disease had involved the 2nd, 3rd and 4th cervical vertebrae; the bodies of the 2nd and 3rd showing signs of fusion and bone regeneration. It is at this point in July 1950, two years after first being admitted, that the child was allowed to 'get up'.
This patient was discharged in December 1950, as being clinically and radiologically inactive and able to dispense with the splint. She continued to be seen as an outpatient at Stannington until 1956. Her last out-patient report stating that there was no deformity and no limitation of movement. Sound fusion was noted between both the vertebral bodies and posterior articulation of the 2nd, 3rd and 4th cervical vertebrae.
Click Images to Enlarge
|
|
AGE : 3
SEX: FEMALE
ADMISSION : 17th Sep 1948
DISCHARGE : 18th Dec 1950
DIAGNOSIS: TB of cervical vertebrae


|