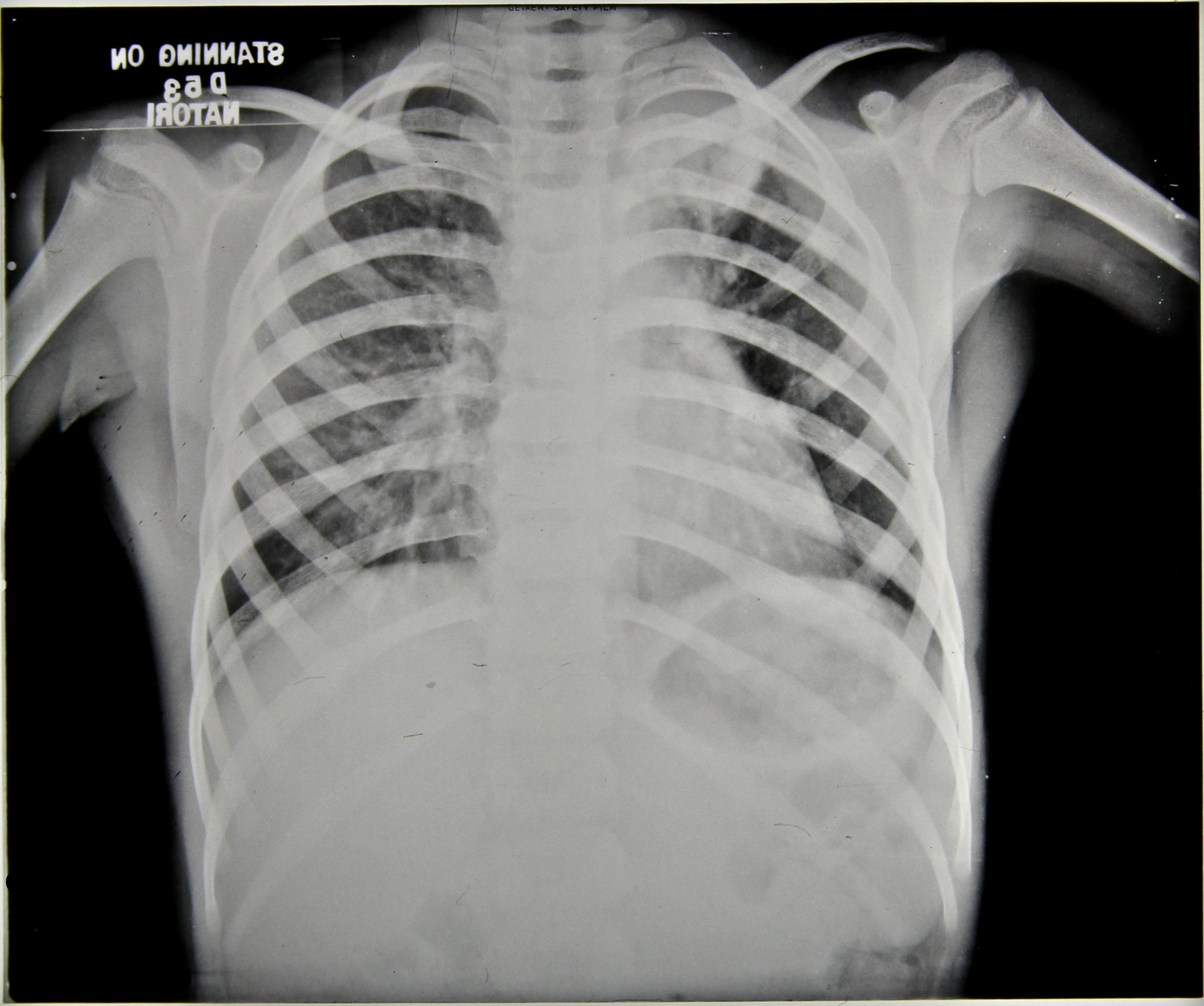
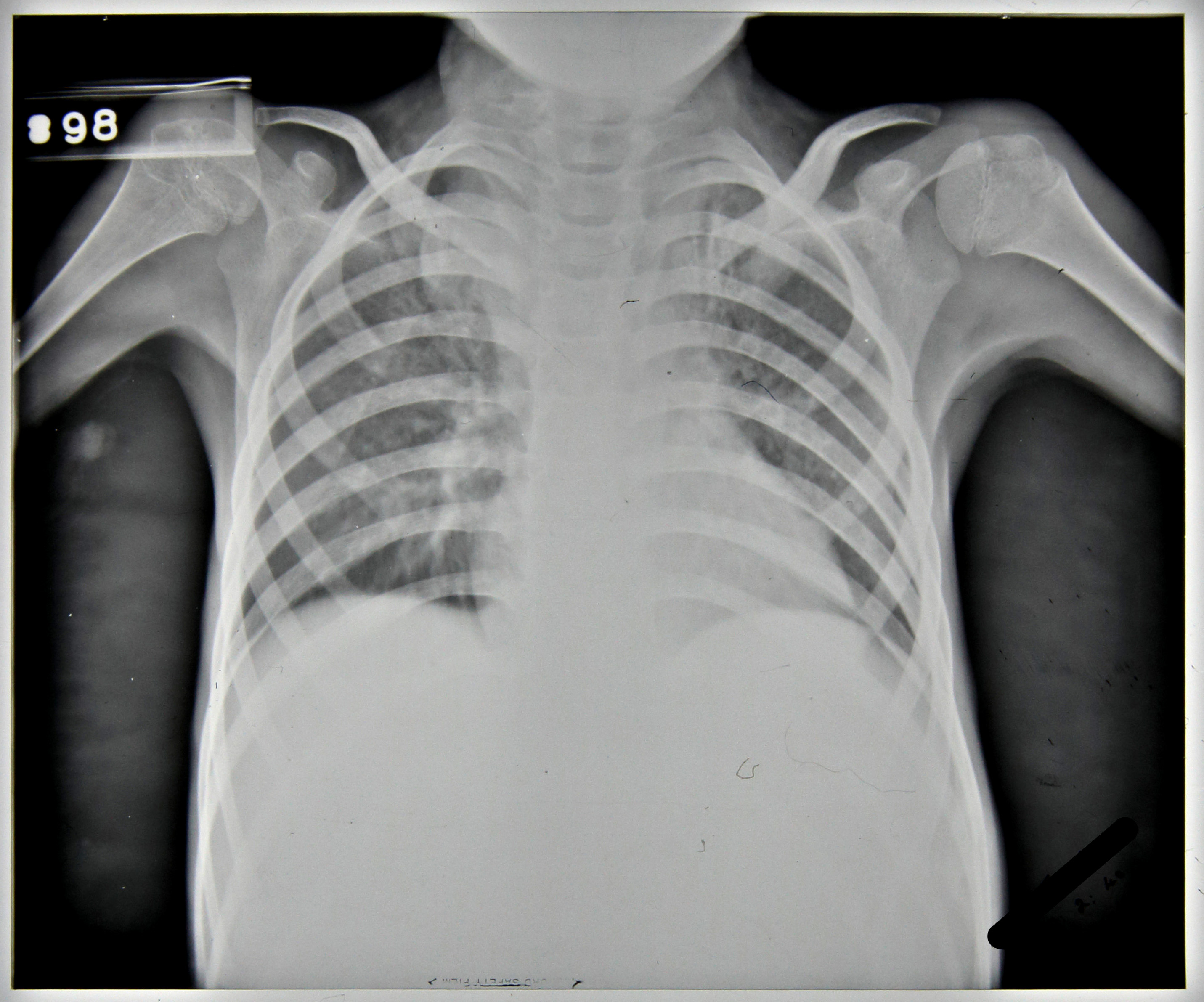
Patient 81/39, a five year old boy, was admitted to Stannington in December 1937 due to ailing health following a two month period in bed suffering from mumps. He had developed a cough, was easily tired and was losing weight. The initial x-ray reports detail a blocked apex in the left lung and marked mottling in the right lung leading to an initial diagnosis of Pulmonary TB, Figure 1. However, following his admission further symptoms started to manifest themselves which indicated that the diagnosis of this patient was more complex than it was initially considered to be.
In April 1938, it was noted the patient had two subcutaneous abscesses on the iliac crest and the knee. A sample of the mucus taken from the abscess on the hip was sent for bacteriological examination. Results of this testing were as follows:
‘scanty pus cells and much granular debris. No definite organisms seen and tubercle bacilli not found.’
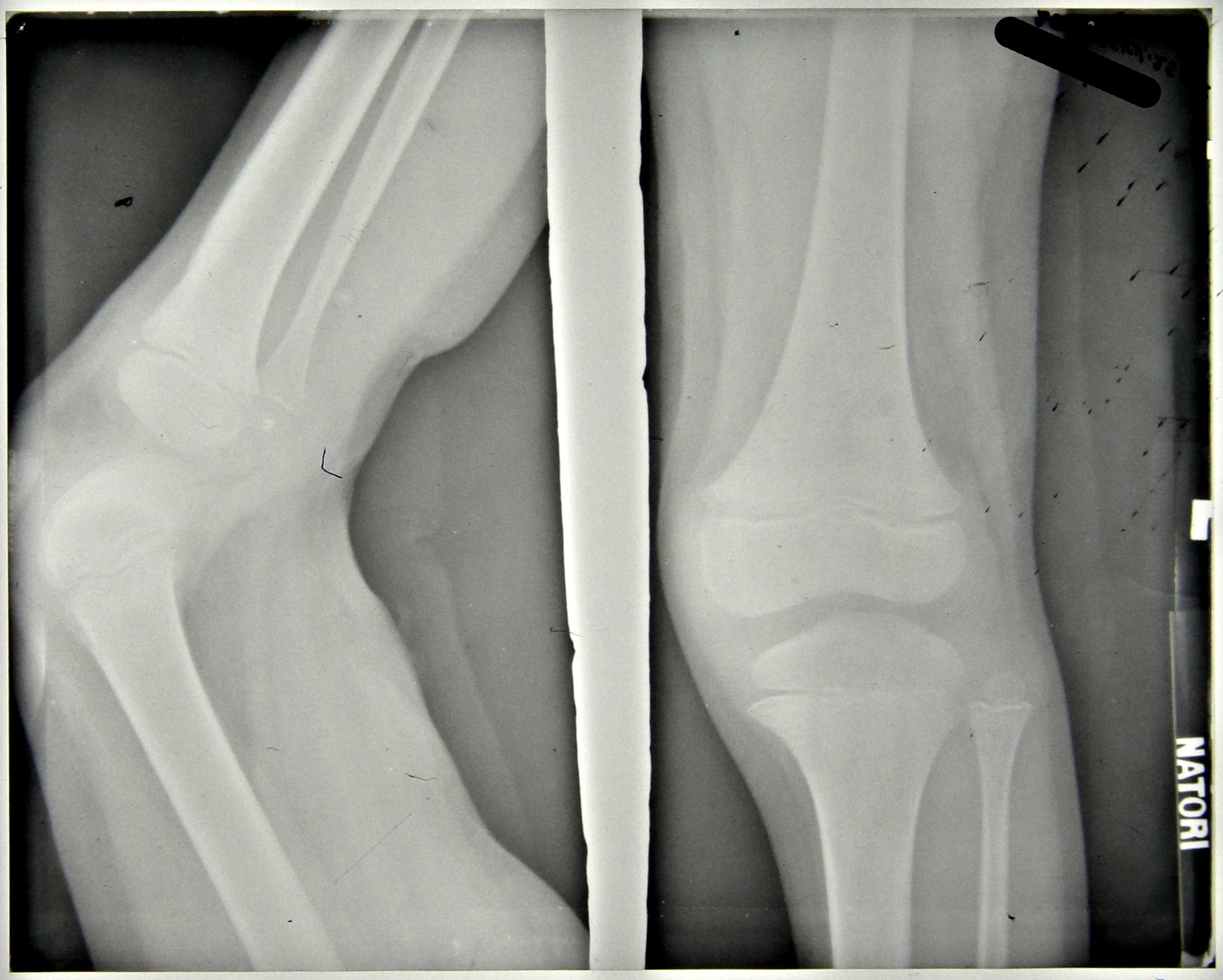
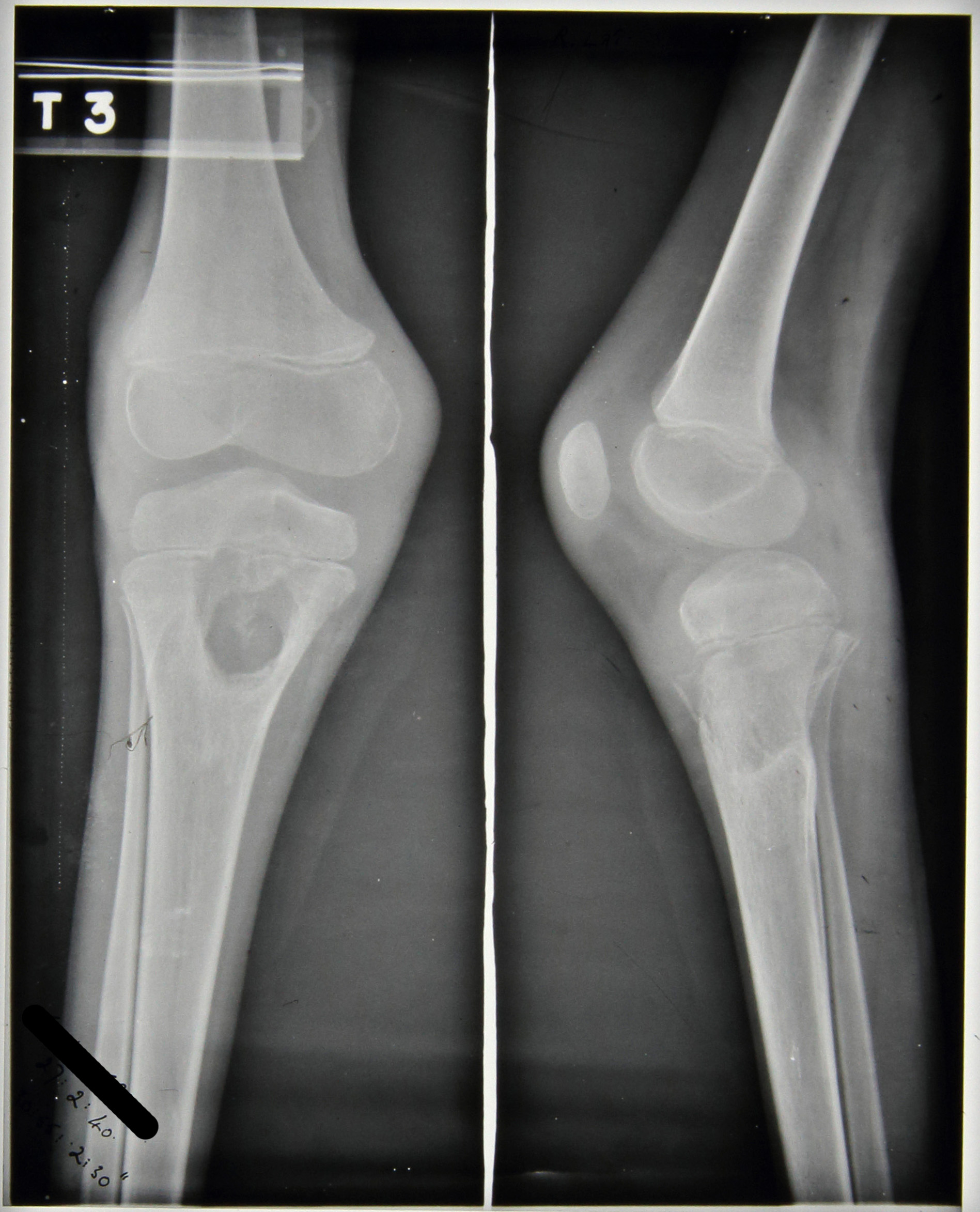
Furthermore, periostitis was noted in the upper end of the ulna which ‘appears septic’ but was regarded as being non-tuberculous. The patient still suffered with a cough but sputum tests were negative and notes state that no tuberculosis was seen. At this stage the x-ray report indicates that no bone lesions are seen in either the leg or the iliac crest, Figures 2 and 3.
Throughout the rest of 1938, the patient’s condition is very variable. An additional abscess is noted in the lumbar region with slight discharge and the apex of the left lung becomes more blocked with the lower lobe of the right lung being described as having been ‘studded with deposits’, however, the sinuses in the thigh and gluteus region are healed.
The main focus of the notes centre upon the right elbow which, in September 1938, was described as being very active with discharging abscesses; periostitis was greatly increased in the ulna and also present in the humerus with the joint being ‘badly involved’, see Figure 4. In November 1938 large sequestrum was removed from the elbow, at this time all lesions were considered very active. The elbow continued to be active with an increasing number of ulcers noted to have appeared; a maximum of four seen in February 1939 including one in the right cubital fossa which is incised to produce ‘copious…pus’, Figure 5.
X-ray reports from September 1939 read as follows:
11/9/39 – Ulna hollowed out to cavity
Radius dislocated upward & forward
Lower end humerus eroded & partly destroyed.
15/9/39 – Ulna – upper end partially destroyed, disorganisation of elbow joint’
No further comment is made regarding a diagnosis of tuberculosis in the elbow.
In addition to ongoing changes in the elbow an abscess appeared on the right mastoid, which was opened and drained in October 1938 and is noted to have become less active by November 1938. However, this abscess continued to open throughout the patient’s stay at Stannington and is often referred to as ‘discharging freely,’ with a diminishment in its activeness finally being noted in October 1939.
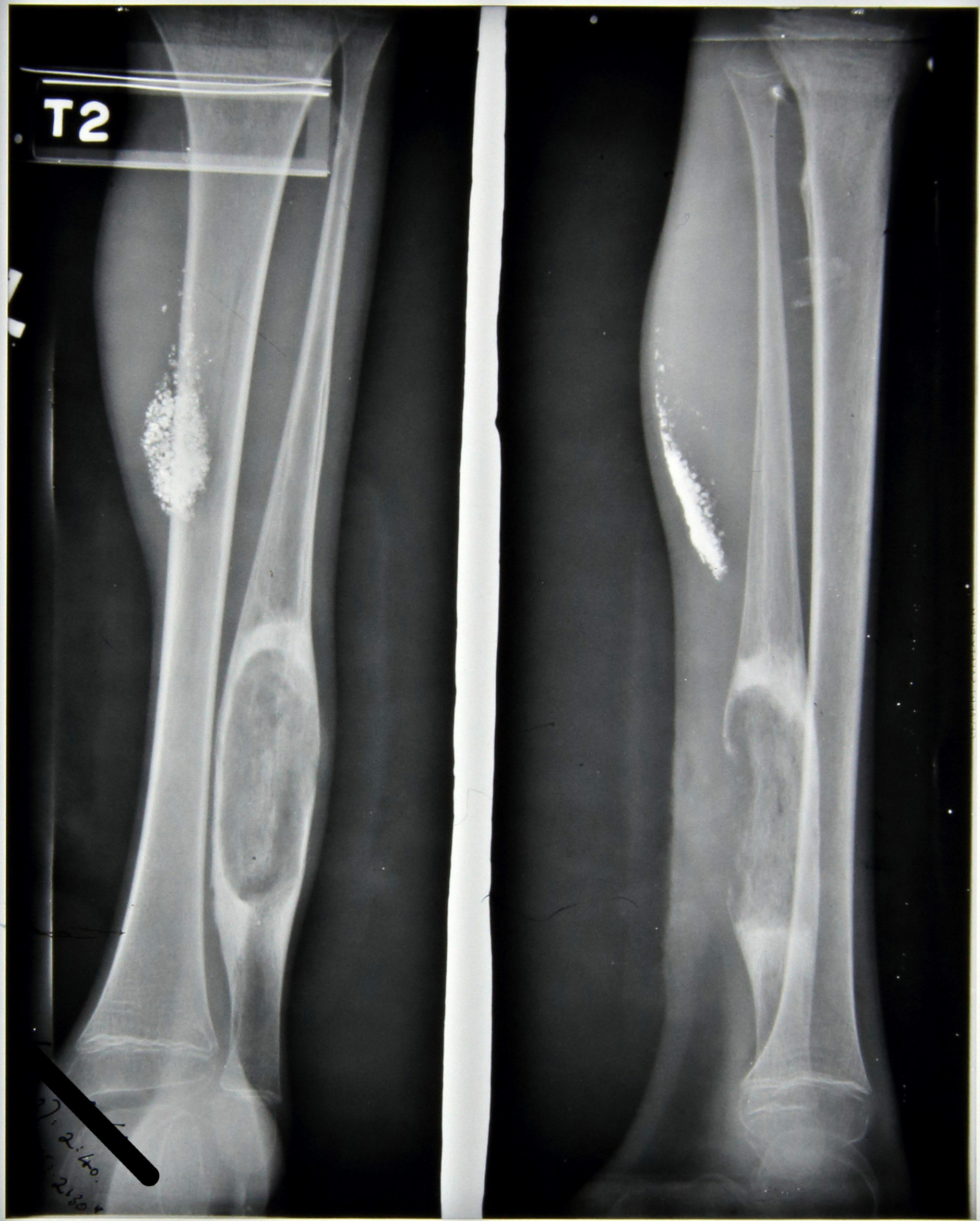
Further skeletal changes are observed in the x-ray report notes from September 1939, Figures 6 and 7:
11/9/39 – Leg – large cavity in fibula L and in head of R. tibia
15/9/39 – Left fibula large focus
Right tibia large focus passing through into epiphysis.
Combined with this the medical notes indicate that a sinus developed on the left ankle and another on the right tibia during the same period with a further sinus developing in November 1939.
This patient was transferred from Stannington in February 1940 to a local hospital in West Hartlepool, his home town, as showing No Medical Improvement and a final diagnosis of TB Bones and Joints and old lung lesion. His final x-ray report, see Figures 8-12, dated 27th February 1940, reads:
‘Large cavity head of R.tibia & sequestrum seem smaller than 11/9/39
The multifocal nature of this patient coupled with comments throughout the notes on possible non-TB origin is suggestive of a potential differential diagnosis. Any further comments based upon the information provided and radiographic images would be welcomed.
‘Escaping from the Kaiser’ by H.W. Tustin is published by Pen & Sword Books.
In the spring of 2013, I came across a dusty old manuscript at my mother’s house in Somerset. It turned out to be my grandfather’s memoir, written about his experiences during the Great War. Reading it was quite a revelation. Not only was it dramatic and well written, but also a fascinating historical document, providing a thorough and vivid description of life in a WWI German PoW camp – an aspect of history that has, I have subsequently discovered, been little explored by historians. I decided to try to have it published, hoping that it might appear in print while the author’s daughter, my now 85-year-old mother, was still around to read it. I am pleased to say that the memoir – ‘Escaping from the Kaiser’ by Herbert Tustin – has just been published by Pen & Sword Books, much to the delight of my mother.
My grandfather’s memoir begins with him in Northern France in April 1915, en route to the Second Battle of Ypres with his regiment, the 8th Durham Light Infantry. He describes how the initial mood of ‘glorious adventure’ gave way to much darker emotions as they neared the battle zone and the grim realities of war become ever more apparent. The 8th Durhams were sent to the most critical section of the allied line, the extreme head of the Ypres Salient. Outgunned and outnumbered, their position was hopeless. The regiment was decimated by the German bombardment, and those that survived were forced into a desperate retreat, during which my grandfather was captured, along with a great many of his comrades.
Following capture, my grandfather and his fellow captives endured an arduous three-day rail journey in cattle trucks to Rennbahn PoW camp, just outside the German city of Münster. Here he was to spend 16 months, and a large portion of his memoir is devoted to describing this experience in great detail: the hunger, hardships and brutalities; the prison work; the character of the various nationalities; the activities and recreations; and the friendships and humour.
Reunited sweethearts Herbert and Sybil. This photo was taken after Tustin’s escape, just outside his family home in Ponteland, Northumberland, England.
Conditions at Rennbahn were tough, but my grandfather made the best of the situation, participating in many of the prisoner-organised activities, including accompanying at the piano for theatrical productions, playing the organ during church services and helping to edit the PoW church magazine. Nevertheless, thoughts of escape ran constantly in his mind. According to a recently acquired recording of an interview with his friend and 8th Durham comrade, Private William Stephenson (1894–1995), my grandfather decided to escape because he got word that a ‘young lieutenant’ was paying too much attention to his sweetheart Sybil, which troubled him greatly and made him determined to return to England as soon as possible. He had met Sybil, who was to become his wife, while they were both trainee teachers at the College of St Hild and St Bede in Durham, and their relationship was kept alive during the war through a frequent exchange of letters.
Whatever mix of emotions inspired my grandfather, they must certainly have been very strong, as attempting to escape was an incredibly risky venture: Rennbahn was surrounded by a triple girdle of barbed wire, with the middle wire carrying a lethal electric charge. Armed guards were posted at every entrance, and watch-dogs patrolled the perimeter fence, which was illuminated by powerful arc lamps. Any would-be escapee who succeeded in breaking free from the camp still needed to cross 50 miles of enemy territory before reaching the safety of neutral Holland. In addition to these formidable difficulties, my grandfather had the sobering knowledge that all previous British escape attempts had failed, and that he would be severely punished if caught. Finally, as if he needed reminding of the dangers, within less than a month of making his own bid for freedom, a French prisoner was shot and killed in the act of attempting to escape.
Rennbahn PoW camp: a view overlooking one of the four blocks. The trees in the distance could not be seen by the prisoners, for no windows opened onto the outside. Rennbahn, one of nearly 300 German PoW camps, was a fairly typical ‘Mannschaftslager’ (a camp for ordinary soldiers rather than commissioned officers) and held as many as 10,000 prisoners of many different nationalities.
My grandfather’s first effort to escape was by tunnelling out of the camp. He and an 8th Durham comrade, Private Thomas B. Dickinson (called ‘Hicky’ in my grandfather’s memoir), also an alumnus of Bede College, took over a tunnel that had been abandoned by other prisoners. They set to their digging work with great enthusiasm, but the increasing moisture and stench, which they suspected was coming from the camp sewers, forced them also to abandon the tunnel.
Not to be defeated, in the summer of 1916, my grandfather conspired with Canadian PoW Gerrie Burk on an alternative plan: this involved cutting the wire beneath one of the entrance gates, which were not electrified but kept under constant armed guard. The idea was to choose a stormy night, wait for the sentry to disappear into the shelter of his box, less than four yards from the gate, creep up, cut the wires and crawl beneath the gate to freedom. It is difficult to see how this audacious plan could have succeeded, but the fact that they were resolved to carry it out says a lot about their determination and courage.
Fortunately, they came up with a better plan: on the pretext of visiting some sick friends, they inveigled their way into the camp hospital, which was just outside the main camp and away from the electric wire. Here they were helped by their PoW friends, one being Private Alfred J. Cleeton (of the 7th Canadians), who by good luck had befriended the watch-dog and was thus able to keep it at bay. Seizing their moment and with the sentries only yards away, the intrepid duo made their dash up and over the ten-foot barbed wire, lacerating their hands horribly in the process, before making good their escape.
For the next nine days they headed for Holland, travelling by night and hiding during daylight hours. Increasingly weak and hungry, they supplemented their small food supply with whatever they could find – wild berries, vegetables foraged from fields and apples stolen from orchards. Each day of their nerve-wracking journey brought new dangers: roving hunters, barking dogs, road blocks, treacherous bogs, children at play and even run-away bulls – all of which threatened to expose their presence and bring their dreams of freedom to an abrupt and inglorious end. Somehow, they managed to avoid recapture, despite the closest of calls. Exhausted almost beyond their ability to continue and only yards from neutral territory, they were met by a fusillade of shots fired at them by German frontier guards. Luckily, it being night-time, they managed to evade the guards and, finding sanctuary in a ditch, crawled slowly forwards, inching past a German sentry before finally crossing the Dutch border to safety and freedom.
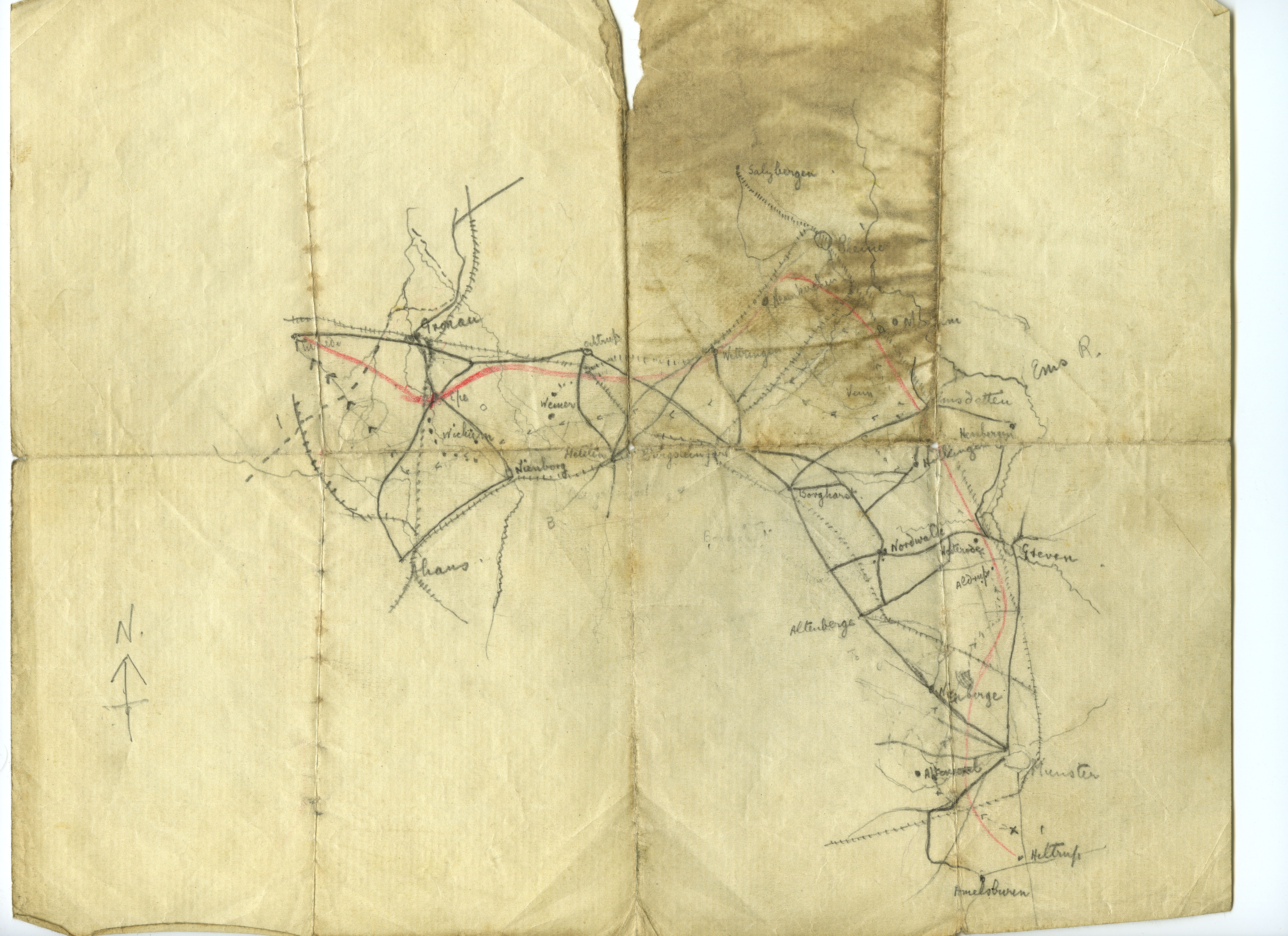
The original pencilled escape map. It is remarkable that this map, drawn on thin, poor quality paper, survived the arduous ten-day escape journey. It is yet more remarkable that it still exists, a century after its creation.
On arriving in Holland, they were relieved to meet a friendly group of soldiers, who accompanied them to the nearby town of Enschede. The Dutch authorities, having verified their story, treated them with the utmost kindness and sent them under escort to Rotterdam, where the British Consul arranged their passage on the first boat leaving for England. Their voyage was a perilous one, for the previous four ships to leave Rotterdam had been torpedoed by German U-boats. Fortunately, their vessel, the SS Grenadier, was able to navigate its way across the mine-strewn, submarine-infested North Sea, to arrive safely in Newcastle on Tyne on 18 September.
My grandfather’s amazing story of war, imprisonment, survival and escape, enhanced by original photographs, concludes with an epilogue by my grandmother. Writing some 20 years after her husband’s death, she recalls his welcome home, the joyful reunion and his proposal of marriage.
Herbert Tustin with his family – wife Sybil, daughter Lynette and son Graham – in Teesdale, c.1936.
Tustin as an officer cadet in 1917. After his escape, he received a commission and was posted to garrison duty in South Africa, where he served out the rest of the war.
Sadly, I never knew my grandfather, whose life was cut short when he died of cancer in 1939. I am grateful, however, that he left such a dramatic and wonderfully written wartime memoir. Having it published has been something of a personal tribute, and I am proud to be related to a man who showed such courage under so much adversity. I am also delighted that that his story – ‘Escaping from the Kaiser’ by Herbert Tustin – is now available to be read and enjoyed by everyone.
We would like to express our sincere appreciation to Richard Corr [grandson of Herbert Tustin] in supplying this article for the Northumberland At War Project.
Thomas Moffatt Allison was born in 1861 in Guisbrough, North Yorkshire, the son of a mining engineer. He went on to study medicine and appears to have moved to Newcastle in the 1890s and by 1901 is recorded in the census as living and working at Dene House Hospital, a private hospital in Ellison Place, Newcastle.
During this time he was heavily involved with the Poor Children’s Holiday Association (PCHA), the charity behind Stannington Sanatorium, holding the role of Honorary Physician to the PCHA and sitting on its General Management Committee. Through his position within the charity he was instrumental in the establishment of the sanatorium at Stannington, which is clear from the annual reports of PCHA. In the 1906 annual report Dr Allison explains what is currently being done to tackle tuberculosis in the area as well as detailing the benefits that a sanatorium at Stannington will bring:
“Speaking of consumption, we have had quite a number of examples of local tuberculosis (bone and gland cases), and also of lung tuberculosis (or consumption), during the year. These we have provided for as well as we could, – having regard to the danger of infecting others if sent to homes where there are other children – that is to say, we have isolated them as far as possible, and provided sputum flasks, etc.
But to cope properly with consumptive children there must be a proper place for them. And we are indeed glad that next Spring our Stannington Sanatorium – (the first in England) for Consumptive Children, will be ready for opening.” [HOSP/STAN/1/3/2]
Patients and Staff Outside the Sanatorium c.1920s [HOSP/STAN/11/1/54]
Once the sanatorium opened in 1907 his close involvement with institution continued as he took on the role of visiting physician and quite clearly held the sanatorium and its young patients close to his heart. The matron in July 1916 made the following comments about a visit he made:
“Dr Allison brought out with him a gentleman to look over the Institution – he also gave me £1 to buy something for the children & has promised to send us records for our gramophone.” [HOSP/STAN/2/1/1]
Various reports on the early days of the Sanatorium along with newspaper articles from the time show Dr Allison to have been a consistent presence in some of the day to day operations of the Sanatorium and not just the medical side of things. His presence at social events and in children’s Christmas parties is reported upon on several occasions.
During his career he wrote extensively on the treatment of tuberculosis and childhood disease with many articles and letters published in the British Medical Journal. He was also active in other areas of local society and was the President of Newcastle Rotary Club and also stood for parliament as a coalition candidate for Morpeth Borough, but was unsuccessful in this particular political venture.
He died in Newcastle on 9 October 1928 leaving a widow, Frances Sarah Allison. His son Gordon, a Lieutenant in the 1st King George’s Gurkha Rifles predeceased him having died in action in north-west India on 8th June 1919 aged 20.
Sources:
‘A Nation of Workers. Will a Nobler Understanding Arise from Comradeship?’, North-Eastern Daily Gazette, 4 Nov 1916
‘Northumberland. Vigorous Contests Anticipated.’ Yorkshire Post and Leeds Intelligencer, 20 Nov 1918











![Patients and Staff Outside the Sanatorium c.1920s [HOSP/STAN/11/1/54]](http://www.northumberlandarchives.com/wp-content/uploads/2015/01/HOSP-STAN-11-01-54.jpg)