|
Patient 2/1946
The most common treatment identified in Stannington for pulmonary tuberculosis was the surgical procedure of artificial pneumothorax. It was performed on patients with advanced disease with the intention of resting the affected lung and hopefully collapsing any cavities at the same time whilst preventing any further spread as a collapsed lung was less likely to spread bacilli. The procedure had been shown to have a marked improvement in the size of tuberculous cavities but could at the same time be a dangerous procedure with a risk of air embolisms, pleural shock, sepsis, emphysema and effusion.
A needle would be inserted through the chest wall to allow for the insertion of air into the pleural cavity. The amount of air inserted would depend on the size of the patient as well as how much the physician in charge though the patient could realistically manage in one go and how quickly they wished the lung to collapse. Once inserted the pressure from the air would force the lung to collapse in on itself and to cease functioning properly. The entire lung would not necessarily be collapsed at once, either because it wasn't necessary for treatment or because fibrotic adhesions between the lung and the chest wall as a result of the disease prevented it from doing so. Where only part of the lung was affected it would not be desirable to collapse the whole lung and in such instances just one lobe might be collapse. Bilateral artificial pneumothorax was also a possibility, whereby part of both lungs would be collapsed at the same time. A state of collapse could be maintained for a period of months or even years and required the patient to undergo regular refills of air in order to do so.
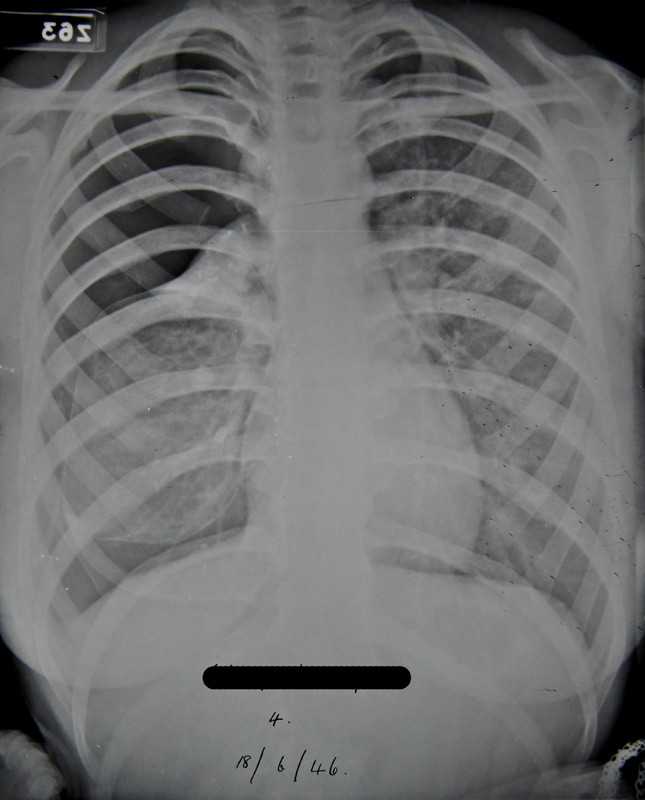
Patient 2/1946 was on such individual to have undergone artificial pneumothorax. A report on an x-ray taken pre-admission reads: "Right lung shows several active foci beginning to coalesce. There is extensive infiltration in the upper zone & suspicious blotchy areas in the middle zone. A small calcified opacity in the right lower zone. The left lung shows infiltration in the middle zone. The upper zone and apex are clear. Early active foci are noticeable in both lungs in the affected areas."
Three months later in June 1945, observations from this boy's x-rays noted: "Scattered foci in right upper zone. One definite cavity. Increased bronchial marking at both bases."
It was quickly decided that and artificial pneumothorax should be induced on the right side and this took place on 16 Aug 1945.
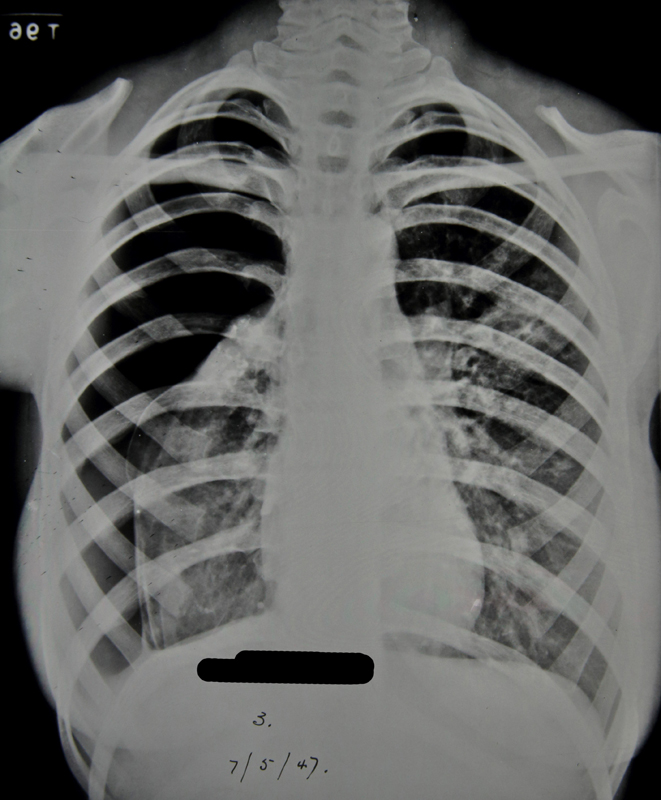
The collapse was maintained well into 1947 which involved her having refills of air every two weeks throughout this period. For the first three months she received refills of 200-300ccs of air at a time, progressing to 400ccs the month after, and then eventually 500-600ccs at a time. This process can be seen in the x-rays provided.
|