Many of the children admitted to the sanatorium came from impoverished backgrounds and had poor living conditions, nearly certain to be a contributing factor to them contracting TB. Some of the common risk factors for contracting tuberculosis include overcrowding, malnourishment, a weakened immune system, being either very young or very old and a lack of access to medical care to ensure treatment and prevention. Consequently, the following account from the records of Stannington Sanatorium hardly comes as a surprise and is by no means unusual.
This particular case from the 1940s perfectly illustrates the challenging conditions and the effect of childhood diseases. The girl, patient 145/1946, was admitted to Stannignton Sanatorium in October of 1945 at the age of 3. Her case notes indicate that she had already had measles and pneumonia and had been suffering from her present condition of tuberculosis of the right knee for the past 18 months. After 4 years of treatment she was considered fit for discharge at which point the living conditions she had left behind at the age of 3 are made clear. The local medical officer reports that
“The home conditions in this case are appalling. The housing accommodation is only two rooms, in which are already living four adults and five children.”
With this borne in mind the medical staff, unsurprisingly, consider it counterproductive to discharge the girl home and within 3 months she is instead discharged to the Briarmede Nursery in Gateshead. Medical staff were obliged to take into consideration the living conditions of all patients and consult with local medical officers in the relevant districts before discharging their patients or risk undoing much of the good that had been achieved during the child’s stay in the sanatorium. Where conditions were not satisfactory children could be discharged to other institutions, as above, or could find themselves staying at the sanatorium longer than was medically necessary, a situation which the doctors were obviously keen to avoid.
For many children coming from backgrounds such as this, being removed to the sanatorium, whilst it may have been difficult being separated from family at such a young age, may in fact have been a blessing in disguise. Even without the effective drug treatments we have today, the instant improvement in living conditions would have made untold differences to their health and wellbeing. In each child’s case file it is quite common to see descriptions of their living conditions in their general and family history, taking into account the type of house they were living in, the number of occupants, and the sanitation available. This information alongside correspondence from the children’s parents requesting support for applications for improved housing gives us a great insight into some of the social conditions across the North East during this period.
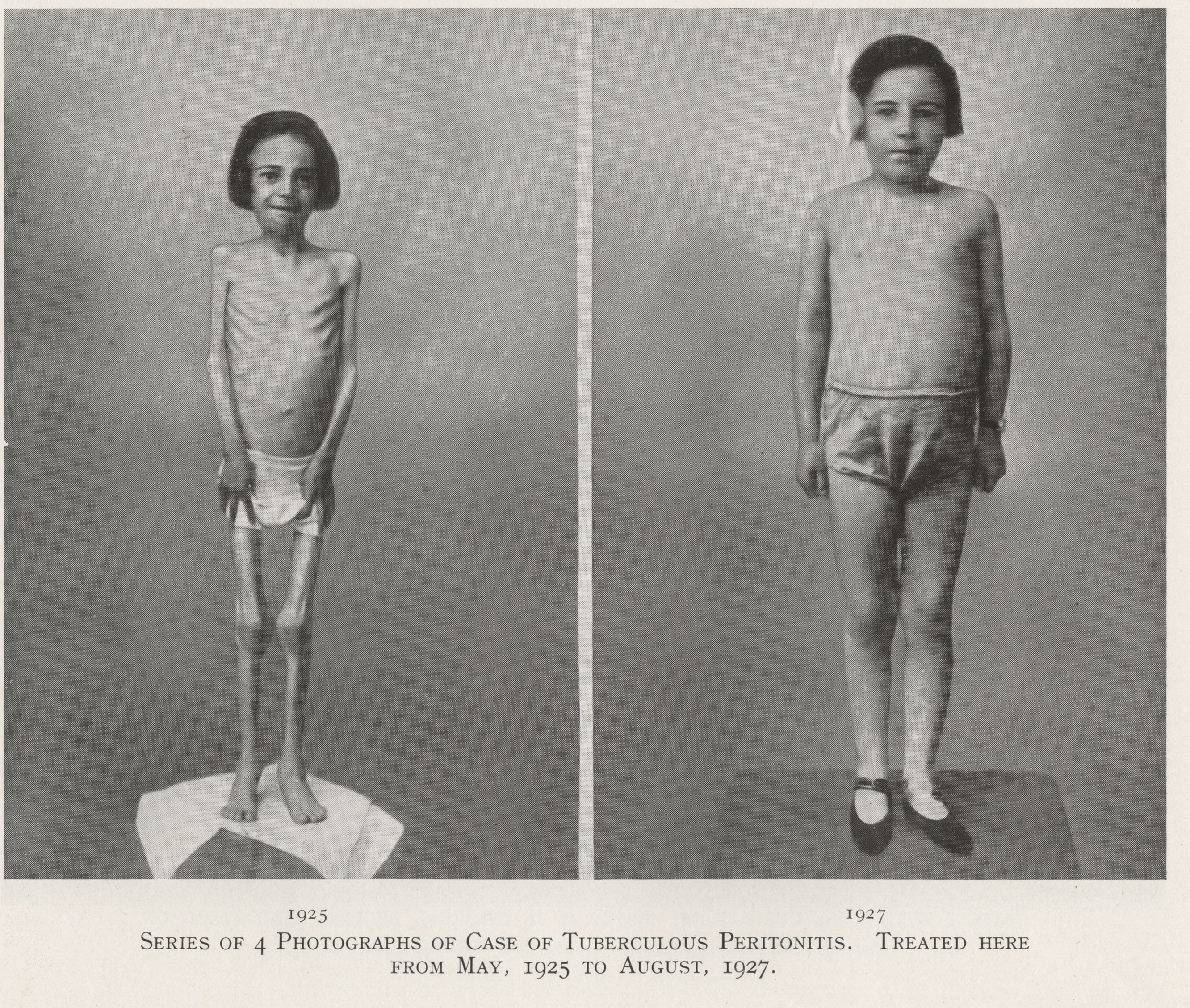
The image below is taken from a brochure produced by the sanatorium in 1936 to promote their services and show images of one patient at four different points in time to illustrate the success of the treatment that Stannington provided. (HOSP/STAN/9/1/1)

See also our later post on Harris Lines.



{kind=link}