Amongst the many collections held by Northumberland Archives are records of the Ridley family of Park End, an estate in the Tynedale area of Northumberland. One of our project volunteers has looked at letter books of the estate and has prepared this short blog about the effect the war had on the estate. Throughout our project we will be examining records that look at the impact the First World War had on the home front in Northumberland.
The estate letter books for the war period start in January 1916 [Ref: – NRO 3386/20-24] when John Farbridge took over as Agent. Charles Noel Ridley inherited the estate on the death of his father, John Hilton Ridley, but died from injuries on active duty in France on 7 October 1915 and was succeeded by his younger brother Arthur Hilton Ridley who had been invalided out of the Army.
The letters show the difficulties of running a large estate during the War. There were regulations about everything. They were told how many fields had to be ploughed for crops and how many left grass for cattle and sheep. Permits had to be obtained for selling hay and straw (if caught selling without a permit people were prosecuted and fined), for obtaining spare parts for farm machines, etc.
Men were being called up despite the war effort to grow food and no exemptions allowed. Women were being employed as Land Army Girls and John Farbridge acknowledges their contribution in one letter. A Rat Catcher was employed to deal with a plague of rats eating the bags of oats, etc. before they could be shipped out, but although he killed a few hundred they were still a problem!
The life of the family is illustrated in the letters. Arthur worked at Hawthorn Leslie & Co. Ltd. building ships for the Admiralty. One of his sisters, Mary, worked at the War Information Office.
To be continued next week with the story about Charles Noel Ridley & his wife.
We would like to express our sincere appreciation to Jean Wilkinson for supplying this article for our Northumberland At War Project.
Month: March 2015
Surgical Procedures – Tenotomy
This week we’re going to take a look at one of the surgical procedures that was used to treat TB and to counter some of it’s side-effects. A register of operations held within the collection lists a number of different procedures that were carried out on the patients, the majority having been performed by the visiting surgeon Mr Johnston. These procedures were employed predominantly before the advent of effective antibiotics but many of them still continued to be used effectively after the introduction of drug therapies. Over the coming months we will explore a range of different treatments that were employed at Stannington, beginning this week with tenotomy.
The records of Stannington Sanatorium show tenotomy to have been performed on several patients suffering from tuberculosis of the bones and joints. The procedure involved the division of the tendon to lengthen it and would be performed in order to counter deformity caused by the tuberculous disease and increase flexion in a particular joint. The tendon would be divided, with the two sections allowed to pull apart and then allowed to re-heal at the overlap of the two parts thus resulting in a lengthening of the tendon. This is not a procedure exclusive to the treatment of tuberculosis but rather in tackling any disease or deformity that has adversely affected the joint. Patients could find themselves unable to fully flex a particular joint and may be left holding it at an unusual angle owing to muscle contracture and possible subluxation, whereby one muscle pulls more strongly than its counterpart causing partial or complete dislocation of the joint. Following the procedure the affected joint may be put in plaster or splinted to ensure that the tendon heals at the new length and the joint is in the correct position.
Patient 83/39 was one patient that underwent the procedure, in this particular case division of the hamstrings to tackle poor flexion in the right knee. Female and aged 3, patient 83/39 was admitted to the sanatorium on 22 October 1937 with a positive mantoux test and the affected knee described as hot, swollen and having limited flexion. Her pre-admission report reads:
“Fell and after 14 days R knee began to swell and began to limp. Went to Durham County Hosp. & leg was immobilised in plaster 4 times. Typical tub. R knee joint probably synovial type.”
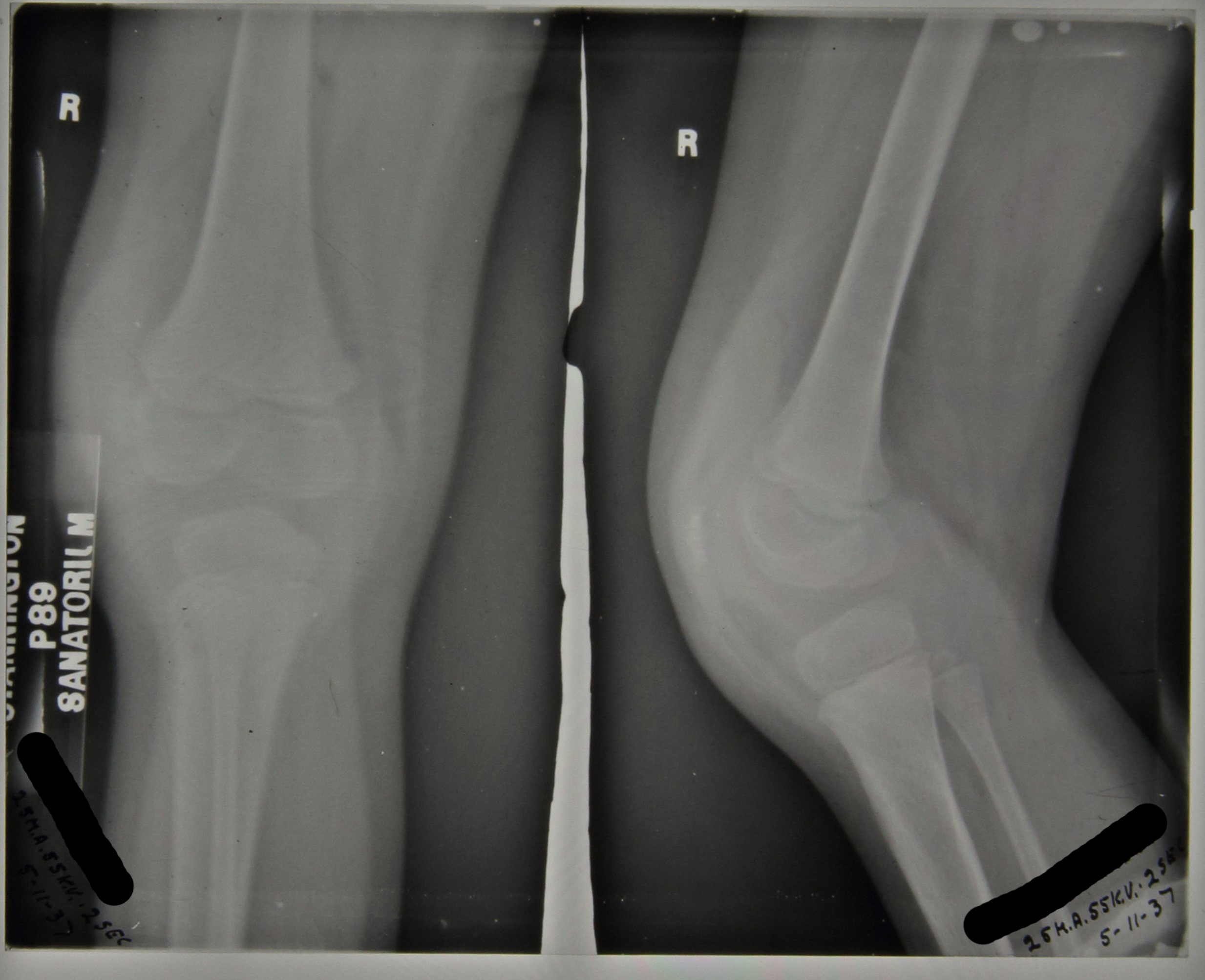
The above radiograph was taken in November 1937, two weeks after admission, with the x-ray report as follows ‘Thickening of capsule. Eburnation and erosion of femoral condyles, especially outer.’
Her progress is noted in her file throughout her stay and in May 1938 it is reported that the flexion in her knee is at 45 degrees and in August 1938 it is decided that she should have her hamstrings divided with the procedure carried out by Mr Johnston on 17 August 1938. There appears to be some initial progress as in September 1938 flexion in the right knee is now reported to be 50 degrees and by October she was wearing a Thomas splint (a traction splint commonly used to immobilise the leg).
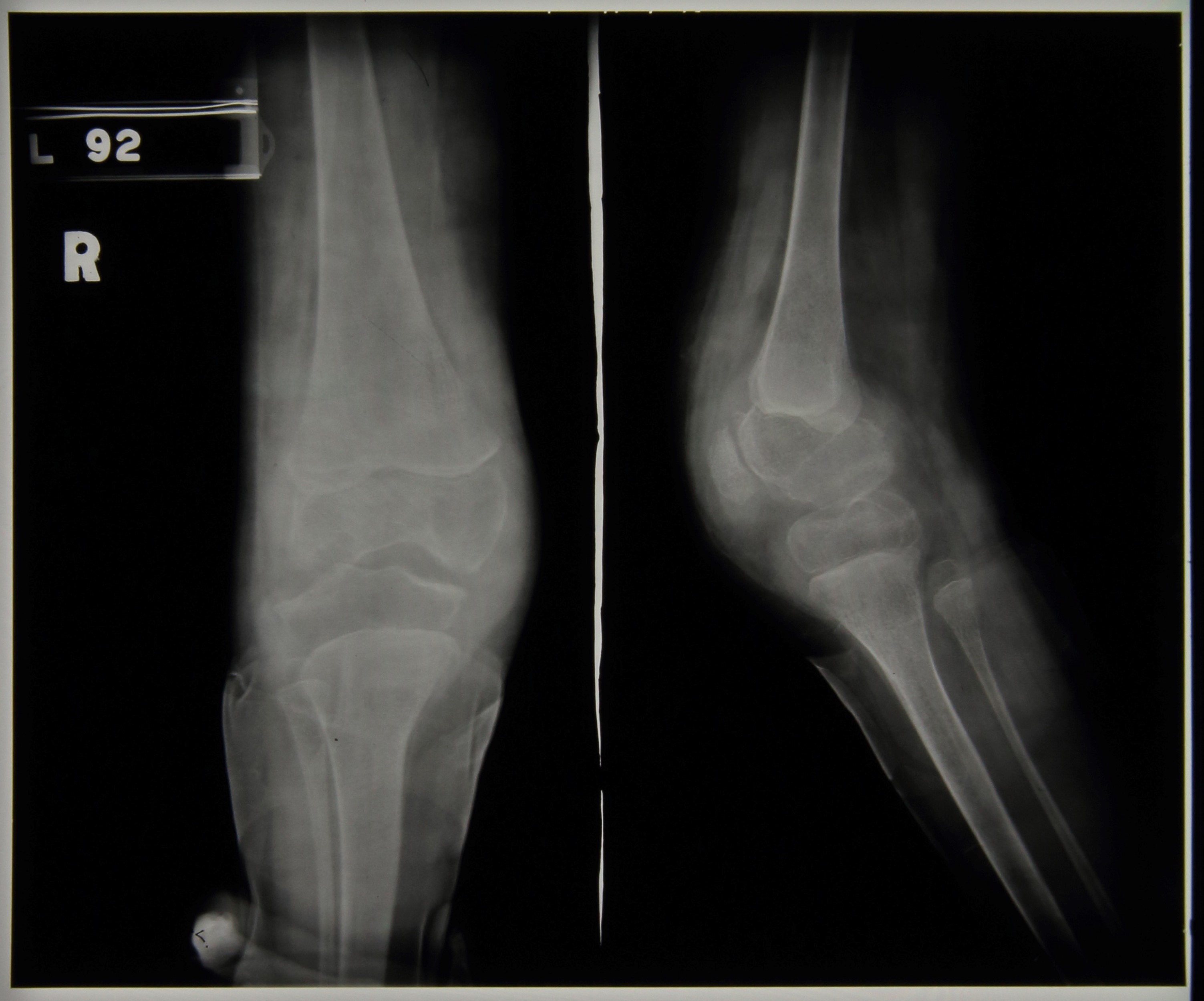
During 1939 progress appeared to be limited with flexion remaining at around 45 degrees throughout, but by January 1940 we see reports that the knee has improved and is almost straight. In April 1940 she was walking well and she was eventually discharged on 9th August 1940 able to walk in a splint. It is debateable as to how much impact the division of the hamstrings had on the eventual straightening of the knee and how much was down to the long term splinting and immobilisation of the joint but she was nonetheless eventually discharged as quiescent. The two radiographs below were taken later on in her stay and date from c.1939/40,

Sources:
J. Krol, Surgery for Deformities Due to Poliomyelitis, (Geneva: World Health Organisation, 1993)